Anterior Cruciate Ligament (ACL) Injuries
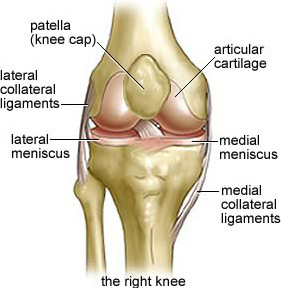
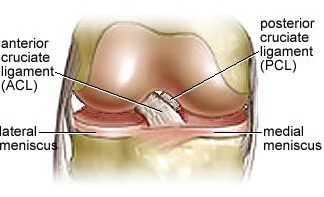
The anterior cruciate ligament passes inside the centre of the knee and connects the femur to the tibia. It acts to guide and constrain the motion of the knee. The ACL is most commonly injured during sports and activities that require twisting, pivoting and rapid stopping and starting.
Following a tear of the ACL patients may feel that their knee “gives way” or feels unstable particularly when they are running, jumping or pivoting. Due to damage at the time of injury and the increased, abnormal movement at the knee following the tear people who have had an ACL injury are more prone to meniscal tears and knee arthritis later in life.
Do I need to have an ACL reconstruction?
Not necessarily. If you have had an isolated ACL tear (no damage to other stabilising structures about the knee) then it is reasonable to trial a period of rehabilitation guided by a physiotherapist. There is some evidence that around half of people will be able to have a knee which feels clinically “stable” enough to resume their previous level of sporting activities with physiotherapy1. This is an interesting summary of the role of physiotherapy[1]. However this is dependent upon the individual’s activity level – the more “active” you intend to be the more you will be asking of your ACL deficient knee.
ACL Reconstruction
During ACL reconstruction a nearby tendon is harvested and then repositioned as a graft inside the knee to recreate the ruptured ligament. Dr Hutchinson utilises both hamstrings and quadriceps tendon grafts. Hamstrings tendons are the most commonly used grafts for ACL reconstruction in Australia. They have a long track record and give reliable results. The quadriceps tendon graft has been in use since the 1980s and gives a larger, stronger reconstructed ligament. Dr Hutchinson has a research interest in quadriceps tendon grafts. The choice of graft is individualised to each patients physiology and requirements. Please feel free to enquire.